Mikrosefalus

Mikrosefalus adalah kelainan otak dengan ukuran kepala lebih kecil dari ukuran kepala rata-rata berdasarkan umur dan jenis kelamin. Kepala dikatakan lebih kecil jika ukuran lingkar kepala kurang dari 42 cm atau lebih kecil dari standar deviasi 3 dibawah angka rata-rata.
Mikrosefalus seringkali terjadi akibat kegagalan pertumbuhan otak pada kecepatan yang normal. Beberapa penyakit yang memengaruhi pertumbuhan otak dapat menyebabkan mikrosefalus. Mikrosefalus seringkali berhubungan dengan keterbelakangan mental. Mikrosefalus dapat terjadi setelah infeksi yang menyebabkan kerusakan pada otak pada bayi yang sangat muda (misalnya meningitis dan meningoensefalitis).
· Penyebab
Mikrosefalus disebabkan oleh gangguan kelainan genetik yang mengganggu pertumbuhan korteks serebral selama bulan-bulan awal perkembangan janin. Hal ini terkait dengan sindrom Down, sindrom kromosom, dan sindrom neurometabolic. Bayi mungkin dilahirkan dengan microcephaly jika selama kehamilan ibu memiliki kebiasaan menyalahgunakan obat-obatan atau alkohol, terinfeksi cytomegalovirus, virus rubela, teracuni bahan kimia tertentu.
· Gejala
Gejala – gejala yang muncul pada bayi:
o Keterbelakangan mental
o Tertunda fungsi motorik dan bicara
o Kelainan wajah
o Perawakan pendek
o Hiperaktif
o Kejang
o Kesulitan dengan koordinasi dan keseimbangan
o Kelainan neurologis
· Perawatan
Tidak ada pengobatan untuk microcephaly yang dapat mengembalikan kepala anak ke ukuran normal atau bentuk. Perawatan berfokus pada cara-cara untuk mengurangi dampak neurologis terkait cacat dan cacat. Anak-anak dengan keterlambatan perkembangan microcephaly dan biasanya dievaluasi oleh pediatrik neurolog dan diikuti oleh tim manajemen medis.
Rakitis
· Penyebab
Penyebab utama dari rakitis adalah kekurangan vitamin D. Vitamin D diperlukan untuk penyerapan kalsium dari usus. Sinar matahari, sinar ultraviolet terutama, memungkinkan sel-sel kulit manusia mengkonversi vitamin D dari aktif ke keadaan aktif. Dengan tidak adanya vitamin D, kalsium tidak benar diserap, mengakibatkan hipokalsemia, menyebabkan cacat tulang dan gigi dan neuromuskuler gejala, misalnya hyperexcitability. Makanan yang mengandung vitamin D termasuk mentega, telur, minyak hati ikan, margarin, susu dan jus, dan ikan berminyak seperti tuna, ikan herring, dan salmon. Suatu bentuk yang jarang dominan terkait-X ada yang disebut rakitis Vitamin D tahan. Kasus telah dilaporkan di Inggris dalam beberapa tahun terakhir dari rakitis pada anak-anak dari latar belakang sosial yang disebabkan oleh ketidakmampuan untuk membuat vitamin D karena sinar ultraviolet matahari tidak mencapai kulit karena penggunaan terus-menerus dari tabir surya yang kuat, atau terlalu banyak "yang mencakup up "di bawah sinar matahari, atau menghabiskan waktu di dalam ruangan terlalu banyak. Kasus lain telah dilaporkan di antara anak-anak dari beberapa kelompok etnis di mana ibu menghindari paparan matahari untuk alasan agama atau budaya, mengarah ke ibu kekurangan vitamin D. British Medical Journal melaporkan pada 2010 bahwa dokter di Newcastle di Tyne melihat 20 kasus rakitis per tahun.
· Gejala
Tanda dan gejala rakitis meliputi:
o Nyeri tulang atau kelembutan
o Masalah gigi
o Kelemahan otot (miopati reyot atau "sindrom bayi floppy" atau "bayi Slinky" (di mana bayi floppy atau Slinky-suka)
o Meningkatkan kecenderungan untuk patah tulang (tulang mudah patah), terutama patah tulang greenstick
o Deformitas rangka
§ Balita: kaki bengkok (genu varum)
§ Anak lebih tua: Knock-lutut (genu valgum) atau "lutut keanginan"
§ Kranial, tulang belakang, dan panggul cacat
o Gangguan pertumbuhan
o Hipokalsemia (tingkat rendah kalsium dalam darah), dan
o Tetani (kejang otot tidak terkendali di seluruh tubuh).
o Craniotabes (tengkorak lunak)
o Costochondral pembengkakan (alias "rosario reyot" atau "rachitic rosario")
o Harrison alur
o Malleoli ganda tanda akibat hiperplasia metaphyseal
o Pelebaran pergelangan tangan menimbulkan kecurigaan awal, itu adalah karena hiperplasia tulang rawan metaphysial.
X-ray atau rontgen dari penderita canggih dari rakitis cenderung hadir dalam cara klasik: kaki busur (kurva luar dari tulang panjang kaki) dan dada cacat. Perubahan dalam tengkorak juga terjadi menyebabkan khas "alun-alun menuju" penampilan. Cacat ini bertahan dalam kehidupan dewasa jika tidak diobati. Konsekuensi jangka panjang termasuk lengkungan permanen atau pengrusakan tulang panjang, dan kembali melengkung.
· Pengobatan
Rakitis dapat didiagnosis dengan bantuan:
o Tes darah:
- Kalsium serum dapat menunjukkan tingkat yang rendah kalsium, fosfor serum mungkin rendah, dan fosfatase alkali serum dapat menjadi tinggi.
o Gas darah arteri dapat mengungkapkan asidosis metabolik
- X-ray tulang yang terkena bisa menunjukkan hilangnya kalsium dari tulang atau perubahan bentuk atau struktur tulang.
- Biopsi tulang jarang dilakukan tetapi akan mengkonfirmasi rakitis.
Pengobatan melibatkan asupan makanan meningkatkan kalsium, fosfat dan vitamin D. Paparan terhadap sinar ultraviolet B (sinar matahari ketika matahari tertinggi di langit), minyak ikan cod, halibut minyak hati, dan viosterol semua sumber vitamin D. Sebuah jumlah yang cukup cahaya ultraviolet B di bawah sinar matahari setiap hari dan persediaan yang memadai kalsium dan fosfor dalam makanan dapat mencegah rakitis. Darker bayi berkulit perlu lebih lama untuk terkena sinar ultraviolet. Penggantian vitamin D telah terbukti benar rakitis menggunakan metode terapi sinar ultraviolet dan obat-obatan. Rekomendasi adalah untuk 400 unit internasional (IU) vitamin D per hari untuk bayi dan anak-anak. Anak-anak yang tidak mendapatkan jumlah yang cukup vitamin D meningkatkan risiko rakitis. Vitamin D sangat penting untuk memungkinkan tubuh untuk penyerapan kalsium untuk digunakan dalam kalsifikasi tulang yang tepat dan pemeliharaan.
Osteoporosis
Osteoporosis adalah penyakit tulang yang mempunyai sifat-sifat khas berupa massa tulang yang rendah, disertai mikro arsitektur tulang dan penurunan kualitas jaringan tulang yang dapat akhirnya menimbulkan kerapuhan tulang.
Klasifikasi:
Osteoporosis primer
Osteoporosis primer sering menyerang wanita paska menopause dan juga pada pria usia lanjut dengan penyebab yang belum diketahui.
Osteoporosis sekunder
Sedangkan osteoporosis sekunder disebabkan oleh penyakit yang berhubungan dengan :
o Cushing's disease
o Hyperthyroidism
o Hyperparathyroidism
o Hypogonadism
o Kelainan hepar
o Kegagalan ginjal kronis
o Kurang gerak
o Kebiasaan minum alkohol
o Pemakai obat-obatan/corticosteroid
o Kelebihan kafein
o Merokok
Osteoporosis anak
Osteoporosis pada anak disebut juvenile idiopathic osteoporosis.
· Penyebab
o Osteoporosis postmenopausal terjadi karena kekurangan estrogen (hormon utama pada wanita), yang membantu mengatur pengangkutan kalsium ke dalam tulang pada wanita. Biasanya gejala timbul pada wanita yang berusia di antara 51-75 tahun, tetapi bisa mulai muncul lebih cepat ataupun lebih lambat. Tidak semua wanita memiliki risiko yang sama untuk menderita osteoporosis postmenopausal, wanita kulit putih dan daerah timur lebih mudah menderita penyakit ini daripada wanita kulit hitam.
o Osteoporosis senilis terjadi karena kekurangan kalsium yang berhubungan dengan usia dan ketidakseimbangan di antara kecepatan hancurnya tulang dan pembentukan tulang yang baru. Senilis berarti bahwa keadaan ini hanya terjadi pada usia lanjut. Penyakit ini biasanya terjadi pada usia diatas 70 tahun dan 2 kali lebih sering menyerang wanita. Wanita seringkali menderita osteoporosis senilis dan postmenopausal.
o Kurang dari 5% penderita osteoporosis juga mengalami osteoporosis sekunder, yang disebabkan oleh keadaan medis lainnya atau oleh obat-obatan.Penyakit ini bisa disebabkan oleh gagal ginjal kronis dan kelainan hormonal (terutama tiroid, paratiroid dan adrenal) dan obat-obatan (misalnya kortikosteroid, barbiturat, anti-kejang dan hormon tiroid yang berlebihan). Pemakaian alkohol yang berlebihan dan merokok bisa memperburuk keadaan ini.
o Osteoporosis juvenil idiopatik merupakan jenis osteoporosis yang penyebabnya tidak diketahui. Hal ini terjadi pada anak-anak dan dewasa muda yang memiliki kadar dan fungsi hormon yang normal, kadar vitamin yang normal dan tidak memiliki penyebab yang jelas dari rapuhnya tulang.
· Gejala
Kepadatan tulang berkurang secara perlahan (terutama pada penderita osteoporosis senilis), sehingga pada awalnya osteoporosis tidak menimbulkan gejala. Beberapa penderita tidak memiliki gejala.
Jika kepadatan tulang sangat berkurang sehingga tulang menjadi kolaps atau hancur, maka akan timbul nyeri tulang dan kelainan bentuk.
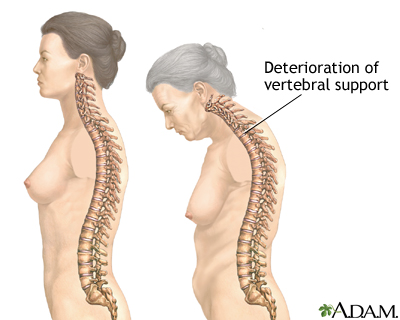
Kolaps tulang belakang menyebabkan nyeri punggung menahun. Tulang belakang yang rapuh bisa mengalami kolaps secara spontan atau karena cedera ringan. Biasanya nyeri timbul secara tiba-tiba dan dirasakan di daerah tertentu dari punggung, yang akan bertambah nyeri jika penderita berdiri atau berjalan. Jika disentuh, daerah tersebut akan terasa sakit, tetapi biasanya rasa sakit ini akan menghilang secara bertahap setelah beberapa minggu atau beberapa bulan. Jika beberapa tulang belakang hancur, maka akan terbentuk kelengkungan yang abnormal dari tulang belakang (punuk Dowager), yang menyebabkan ketegangan otot dan sakit.
Tulang lainnya bisa patah, yang seringkali disebabkan oleh tekanan yang ringan atau karena jatuh. Salah satu patah tulang yang paling serius adalah patah tulang panggul. Yang juga sering terjadi adalah patah tulang lengan (radius) di daerah persambungannya dengan pergelangan tangan, yang disebut fraktur Colles. Selain itu, pada penderita osteoporosis, patah tulang cenderung menyembuh secara perlahan.
· Pencegahan
Pencegahan osteoporosi meliputi:
o Mempertahankan atau meningkatkan kepadatan tulang dengan mengonsumsi kalsium yang cukup
o Melakukan olah raga dengan beban
o Mengkonsumsi obat (untuk beberapa orang tertentu).
Mengkonsumsi kalsium dalam jumlah yang cukup sangat efektif, terutama sebelum tercapainya kepadatan tulang maksimal (sekitar umur 30 tahun). Minum 2 gelas susu dan tambahan vitamin D setiap hari, bisa meningkatkan kepadatan tulang pada wanita setengah baya yang sebelumnya tidak mendapatkan cukup kalsium. Akan tetapi tablet kalsium dan susu yang dikonsumsi setiap hari akhir - akhir ini menjadi perdebatan sebagai pemicu terjadi osteoporosis, berhubungan dengan teori osteoblast.
Olah raga beban (misalnya berjalan dan menaiki tangga) akan meningkatkan kepadatan tulang. Berenang tidak meningkatkan kepadatan tulang.
Estrogen membantu mempertahankan kepadatan tulang pada wanita dan sering diminum bersamaan dengan progesteron. Terapi sulih estrogen paling efektif dimulai dalam 4-6 tahun setelah menopause; tetapi jika baru dimulai lebih dari 6 tahun setelah menopause, masih bisa memperlambat kerapuhan tulang dan mengurangi risiko patah tulang. Raloksifen merupakan obat menyerupai estrogen yang baru, yang mungkin kurang efektif daripada estrogen dalam mencegah kerapuhan tulang, tetapi tidak memiliki efek terhadap payudara atau rahim. Untuk mencegah osteroporosis, bisfosfonat (contohnya alendronat), bisa digunakan sendiri atau bersamaan dengan terapi sulih hormon.
· Pengobatan
Pada seseorang yang mengalami patah tulang, diagnosis osteoporosis ditegakkan berdasarkan gejala, pemeriksaan fisik dan rontgen tulang. Pemeriksaan lebih lanjut mungkin diperlukan untuk menyingkirkan keadaan lainnya yang bisa diatasi, yang bisa menyebabkan osteoporosis.
Untuk mendiagnosis osteoporosis sebelum terjadinya patah tulang dilakukan pemeriksaan yang menilai kepadatan tulang. Pemeriksaan yang paling akurat adalah DXA (dual-energy x-ray absorptiometry). Pemeriksaan ini aman dan tidak menimbulkan nyeri, bisa dilakukan dalam waktu 5-15 menit. DXA sangat berguna untuk:
o Wanita yang memiliki risiko tinggi menderita osteoporosis
o Penderita yang diagnosisnya belum pasti
o Penderita yang hasil pengobatannya harus dinilai secara akurat.
Tujuan pengobatan adalah meningkatkan kepadatan tulang. Semua wanita, terutama yang menderita osteoporosis, harus mengonsumsi kalsium dan vitamin D dalam jumlah yang mencukupi.
Wanita paska menopause yang menderita osteoporosis juga bisa mendapatkan estrogen (biasanya bersama dengan progesteron) atau alendronat, yang bisa memperlambat atau menghentikan penyakitnya. Bifosfonat juga digunakan untuk mengobati osteoporosis.
Alendronat berfungsi:
o Mengurangi kecepatan penyerapan tulang pada wanita pasca menopause
o Meningkatakan massa tulang di tulang belakang dan tulang panggul
o Mengurangi angka kejadian patah tulang.
Supaya diserap dengan baik, alendronat harus diminum dengan segelas penuh air pada pagi hari dan dalam waktu 30 menit sesudahnya tidak boleh makan atau minum yang lain. Alendronat bisa mengiritasi lapisan saluran pencernaan bagian atas, sehingga setelah meminumnya tidak boleh berbaring, minimal selama 30 menit sesudahnya. Obat ini tidak boleh diberikan kepada orang yang memiliki kesulitan menelan atau penyakit kerongkongan dan lambung tertentu.
Kalsitonin dianjurkan untuk diberikan kepada orang yang menderita patah tulang belakang yang disertai nyeri. Obat ini bisa diberikan dalam bentuk suntikan atau semprot hidung.
Tambahan fluorida bisa meningkatkan kepadatan tulang. Tetapi tulang bisa mengalami kelainan dan menjadi rapuh, sehingga pemakaiannya tidak dianjurkan.
Pria yang menderita osteoporosis biasanya mendapatkan kalsium dan tambahan vitamin D, terutama jika hasil pemeriksaan menunjukkan bahwa tubuhnya tidak menyerap kalsium dalam jumlah yang mencukupi. Jika kadar testosteronnya rendah, bisa diberikan testosteron.
Patah tulang karena osteoporosis harus diobati. Patah tulang panggul biasanya diatasi dengan tindakan pembedahan. Patah tulang pergelangan biasanya digips atau diperbaiki dengan pembedahan. Pada kolaps tulang belakang disertai nyeri punggung yang hebat, diberikan obat pereda nyeri, dipasang supportive back brace dan dilakukan terapi fisik.





